Chapter 10: Clinical Settings
Overview
Clinical Settings is where you configure standards, thresholds, and alerts that guide clinical documentation and quality assurance throughout your agency. This chapter covers:
- Documentation standards and timelines
- Vital sign thresholds and clinical alerts
- QA review time thresholds
- System-wide clinical rules and policies
Who Should Read This Chapter:
- Agency Administrators
- Clinical Managers
- Quality Assurance (QA) staff
- Directors of Nursing
Prerequisites:
- Completed agency settings (Chapter 4)
- Understanding of clinical documentation requirements
- Familiarity with Medicare and state regulatory standards
10.1 Accessing Clinical Settings
Navigation Path
- From the Dashboard: Click the Settings icon (gear icon) in the top-right header bar
- Select "Clinical Settings" from the dropdown menu
- The Clinical Settings page will open
What You'll See:
- Three main configuration sections:
- Documentation Standards
- Clinical Alerts & Triggers (Vital Sign Thresholds)
- QA Review Thresholds
- A Save Changes button in the top-right corner (saves all sections at once)
10.2 Documentation Standards
Documentation Standards define the timelines and rules for completing clinical documentation across your agency.
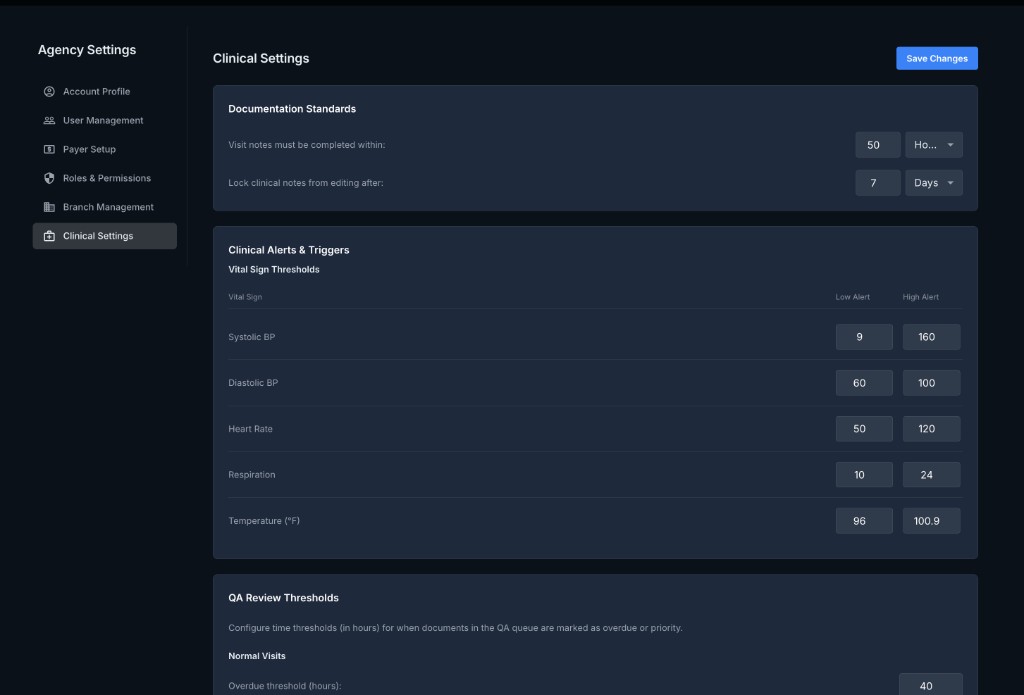
10.2.1 Visit Notes Completion Deadline
Visit notes must be completed within:
- Purpose: Enforces timely completion of visit notes after a visit is performed
- Format: Number + Time Unit (Hours or Days)
- Default: 50 Hours
- Examples:
24 Hours- Visit notes must be completed within 24 hours of the visit48 Hours- Visit notes must be completed within 2 days7 Days- Visit notes must be completed within 1 week
Why This Matters:
- Medicare Compliance: CMS requires timely documentation for reimbursement
- State Regulations: Many states mandate visit notes within 24-48 hours
- Quality Assurance: Timely documentation improves accuracy and care coordination
- Billing: Late documentation can delay claim submission
How It Works:
- A clinician completes a visit in the field
- The system tracks the visit completion timestamp
- If the visit note is not completed within the configured timeframe, the system:
- Flags the visit as Overdue in the clinician's dashboard
- Sends notifications to the clinician and their supervisor (if configured)
- Displays the visit in the QA Center as Pending Documentation
Best Practices:
- Medicare/Medicaid: Set to 24 Hours or 48 Hours to ensure compliance
- Private Payers: Verify payer requirements (some allow 7 days)
- Agency Policy: Align with your internal policies and state regulations
10.2.2 Lock Clinical Notes After
Lock clinical notes from editing after:
- Purpose: Prevents editing of clinical notes after a specified timeframe to ensure documentation integrity
- Format: Number + Time Unit (Days)
- Default: 7 Days
- Examples:
3 Days- Notes are locked 3 days after completion7 Days- Notes are locked 7 days after completion (default)14 Days- Notes are locked 14 days after completion
Why This Matters:
- Audit Protection: Prevents retroactive changes that could raise compliance concerns
- Regulatory Compliance: Many regulators require immutable documentation after a certain period
- Legal Protection: Locked notes demonstrate documentation integrity in legal disputes
- Billing Integrity: Prevents changes to documentation after claims are submitted
How It Works:
- A clinician completes and submits a visit note
- The system tracks the submission timestamp
- After the configured lock period:
- The visit note becomes read-only for all users (except Super Administrators)
- An Edit button is disabled or hidden
- A message appears: "This note is locked and cannot be edited (completed on [date])"
- If edits are needed after locking:
- Option A: Super Administrators can unlock the note (with audit trail)
- Option B: Create an Addendum to the note (recommended for compliance)
Best Practices:
- Standard Setting: 7 Days is a common industry standard
- Shorter Periods: Use 3-5 days if your agency has strict audit requirements
- Longer Periods: Use 14 days if clinicians frequently need to make corrections
- Addendum Policy: Train staff to use addendums instead of editing locked notes
Important Notes:
- Locking applies to:
- ✅ Visit notes
- ✅ OASIS assessments
- ✅ Care orders
- ✅ Clinical documentation
- Locking does NOT apply to:
- ❌ Administrative corrections (typos in patient demographics)
- ❌ Billing adjustments (managed separately)
10.3 Clinical Alerts & Triggers (Vital Sign Thresholds)
Clinical Alerts & Triggers define the vital sign thresholds that generate automatic alerts when patient vital signs fall outside normal ranges during documentation.
10.3.1 Purpose of Vital Sign Thresholds
What Are Vital Sign Thresholds?
- Pre-configured normal ranges for vital signs (blood pressure, heart rate, respiration, temperature)
- When a clinician documents a vital sign outside the normal range, the system:
- Displays an alert (warning or critical)
- Prompts the clinician to acknowledge the abnormal value
- Flags the visit for QA review (if configured)
- Logs the alert in the patient's clinical record
Why Use Thresholds?
- Patient Safety: Ensures abnormal vital signs are noticed and addressed
- Clinical Decision Support: Alerts clinicians to potential emergencies
- QA Monitoring: Tracks patients with unstable vital signs
- Regulatory Compliance: Demonstrates proactive monitoring for state surveys and audits
10.3.2 Configuring Vital Sign Thresholds
Each vital sign has two threshold levels:
- Low Alert - Indicates a value below the normal range
- High Alert - Indicates a value above the normal range
Systolic Blood Pressure (BP)
| Threshold | Value | Meaning |
|---|---|---|
| Low Alert | 9 mmHg | Critically low systolic BP (likely data entry error or severe hypotension) |
| High Alert | 160 mmHg | High systolic BP (hypertension concern) |
Typical Normal Range: 90-140 mmHg
Clinical Interpretation:
- Below 90 mmHg: Hypotension (dizziness, fainting risk)
- Above 160 mmHg: Hypertension (stroke or heart attack risk)
- Above 180 mmHg: Hypertensive crisis (emergency)
Alert Example:
- Clinician enters systolic BP: 185 mmHg
- System displays: ⚠️ "High blood pressure detected. Systolic BP is 185 mmHg (threshold: 160 mmHg). Notify physician if not already aware."
Diastolic Blood Pressure (BP)
| Threshold | Value | Meaning |
|---|---|---|
| Low Alert | 60 mmHg | Low diastolic BP |
| High Alert | 100 mmHg | High diastolic BP |
Typical Normal Range: 60-90 mmHg
Clinical Interpretation:
- Below 60 mmHg: Hypotension (possible perfusion issues)
- Above 100 mmHg: Hypertension (cardiovascular risk)
Heart Rate (Pulse)
| Threshold | Value | Meaning |
|---|---|---|
| Low Alert | 50 bpm | Bradycardia (slow heart rate) |
| High Alert | 120 bpm | Tachycardia (fast heart rate) |
Typical Normal Range: 60-100 bpm
Clinical Interpretation:
- Below 50 bpm: Bradycardia (heart block, medication effect, athletic conditioning)
- Above 120 bpm: Tachycardia (fever, infection, anxiety, heart condition)
- Above 150 bpm: Severe tachycardia (emergency)
Alert Example:
- Clinician enters heart rate: 45 bpm
- System displays: ⚠️ "Low heart rate detected. Pulse is 45 bpm (threshold: 50 bpm). Assess patient for dizziness, fatigue, or syncope."
Respiration Rate
| Threshold | Value | Meaning |
|---|---|---|
| Low Alert | 10 breaths/min | Bradypnea (slow breathing) |
| High Alert | 24 breaths/min | Tachypnea (fast breathing) |
Typical Normal Range: 12-20 breaths/min
Clinical Interpretation:
- Below 10 breaths/min: Bradypnea (respiratory depression, opioid effect)
- Above 24 breaths/min: Tachypnea (respiratory distress, infection, pain)
- Above 30 breaths/min: Severe respiratory distress (emergency)
Temperature (°F)
| Threshold | Value | Meaning |
|---|---|---|
| Low Alert | 96°F | Hypothermia |
| High Alert | 100.9°F | Fever |
Typical Normal Range: 97.0-99.5°F
Clinical Interpretation:
- Below 96°F: Hypothermia (cold exposure, shock, hypothyroidism)
- Above 100.4°F: Fever (infection, inflammation)
- Above 103°F: High fever (serious infection, emergency)
Alert Example:
- Clinician enters temperature: 102.5°F
- System displays: ⚠️ "Fever detected. Temperature is 102.5°F (threshold: 100.9°F). Assess for infection and notify physician."
10.3.3 Customizing Thresholds
To Update Thresholds:
- In the Clinical Alerts & Triggers section, locate the vital sign you want to modify
- Enter the new Low Alert value (left field)
- Enter the new High Alert value (right field)
- Click Save Changes at the top of the page
Considerations When Customizing:
- Agency Policy: Align with your clinical policies and protocols
- Patient Population: Consider your typical patient demographics (e.g., elderly patients may have different normal ranges)
- Physician Input: Consult with your medical director or clinical advisors
- Regulatory Standards: Ensure thresholds meet state and federal guidelines
Example Customization:
- Geriatric Agency: Lower systolic BP high alert from 160 to 150 mmHg (more conservative for elderly patients)
- Cardiac Care Agency: Lower heart rate alerts to catch arrhythmias earlier
10.3.4 How Alerts Work During Documentation
Scenario: A nurse is completing a visit note for a patient.
- Enter Vital Signs:
- Nurse documents: Systolic BP = 185 mmHg, Diastolic BP = 95 mmHg, Heart Rate = 88 bpm
- System Checks Thresholds:
- Systolic BP (185) > High Alert Threshold (160) → Alert Triggered
- Alert Display:
- ⚠️ "High Blood Pressure Alert: Systolic BP is 185 mmHg (threshold: 160 mmHg)."
- Prompt: "Have you notified the physician? ☐ Yes ☐ No"
- Nurse Acknowledges:
- Nurse checks: ☑️ "Yes, physician notified"
- Nurse adds note: "Physician aware. Blood pressure medication adjusted."
- System Actions:
- Alert is logged in the patient's clinical record
- Visit is flagged for QA review (if configured)
- Alert appears in the patient's Clinical Overview and Alerts tab
10.3.5 Vital Sign Alert Best Practices
✅ Do This:
-
Set Conservative Thresholds:
- It's better to alert on borderline values than to miss critical changes
- Adjust thresholds based on your patient population
-
Train Clinicians:
- Ensure all clinical staff understand the thresholds
- Teach proper response protocols (notify physician, reassess patient, document interventions)
-
Review Alerts Regularly:
- QA staff should review all vital sign alerts
- Identify patterns (e.g., multiple patients with high BP may indicate a community outbreak or seasonal issue)
-
Document Actions Taken:
- Always document what was done in response to an alert
- Include: Physician notification, interventions, patient response
-
Use Alerts for QA Monitoring:
- Track which clinicians have the most alerts (training opportunity)
- Identify patients with frequent alerts (may need care plan adjustment)
❌ Avoid This:
-
Don't Set Thresholds Too Wide:
- If thresholds are too lenient, you'll miss important clinical changes
- Example: Setting high BP alert to 180 mmHg misses patients in the 160-179 range (stage 2 hypertension)
-
Don't Ignore Alerts:
- Alerts are clinical decision support tools, not just system noise
- Train staff to take every alert seriously
-
Don't Override Alerts Without Documentation:
- If a clinician acknowledges an alert, they must document the reason and action taken
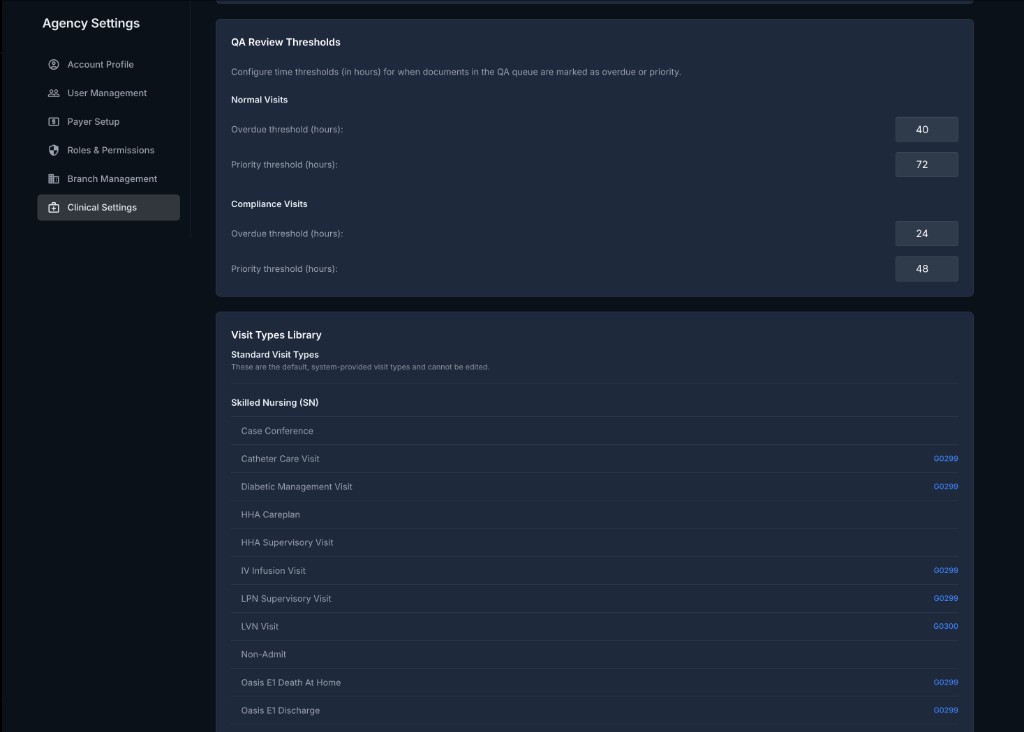
10.4 QA Review Thresholds
QA Review Thresholds define the time limits for QA staff to review and approve clinical documentation before it becomes overdue.
10.4.1 Purpose of QA Review Thresholds
What Are QA Review Thresholds?
- Time limits (in hours) for QA staff to review specific types of documentation
- When a document exceeds the threshold without review:
- It is marked as Overdue in the QA Center
- Notifications are sent to QA staff and supervisors
- The document appears in the Overdue filter in the QA Center
Why Use Thresholds?
- Timely Billing: Ensures documentation is reviewed and approved before claim submission deadlines
- Compliance: Meets Medicare and payer requirements for timely documentation
- Accountability: Tracks QA staff performance and workload
- Patient Safety: Identifies delays in care coordination
10.4.2 Configuring QA Review Thresholds
The system has two main threshold categories:
Normal Visits
These are routine skilled nursing, therapy, and HHA visits.
| Threshold | Value (Hours) | Meaning |
|---|---|---|
| Overdue threshold | 40 hours | If not reviewed within 40 hours, marked as overdue |
| Priority threshold | 72 hours | If not reviewed within 72 hours, escalated to priority |
Typical Timeline:
- 0-40 hours: Normal review period
- 40-72 hours: Overdue (QA staff notified)
- 72+ hours: Priority escalation (supervisors notified)
Use Case:
- A nurse completes a visit note on Monday at 9:00 AM
- QA review is due by Tuesday at 1:00 PM (40 hours later)
- If not reviewed by Tuesday 1:00 PM, it becomes Overdue
- If still not reviewed by Thursday at 9:00 AM (72 hours), it escalates to Priority
Compliance Visits
These are OASIS assessments, recertifications, discharges, and other compliance-critical documentation.
| Threshold | Value (Hours) | Meaning |
|---|---|---|
| Overdue threshold | 24 hours | If not reviewed within 24 hours, marked as overdue |
| Priority threshold | 48 hours | If not reviewed within 48 hours, escalated to priority |
Why Shorter Thresholds?
- OASIS Timing: OASIS assessments must be transmitted to the state within specific timeframes
- Certification Deadlines: Care orders and recertifications have strict Medicare deadlines
- Claim Submission: Compliance visits directly impact billing and reimbursement
Use Case:
- A nurse completes an OASIS Start of Care on Monday at 9:00 AM
- QA review is due by Tuesday at 9:00 AM (24 hours later)
- If not reviewed by Tuesday 9:00 AM, it becomes Overdue
- If still not reviewed by Wednesday at 9:00 AM (48 hours), it escalates to Priority
10.4.3 How QA Thresholds Work
Scenario: QA staff member reviews the QA Center queue.
- Visit Note Submitted:
- Nurse completes a visit note on Monday, 10:00 AM
- Visit enters the QA queue with status: Pending Review
- Overdue Threshold Reached (40 hours):
- By Wednesday, 2:00 AM, if not reviewed, status changes to: Overdue
- QA staff see the visit highlighted in red or with an "Overdue" badge
- Email/notification sent to QA staff: "You have 5 overdue visit notes"
- Priority Threshold Reached (72 hours):
- By Thursday, 10:00 AM, if still not reviewed, status changes to: Priority
- Visit moves to the top of the QA queue
- Email sent to Clinical Manager: "Priority escalation: Visit note from Monday requires immediate review"
- QA Review Completed:
- QA staff reviews and approves the visit
- Status changes to: Approved
- Visit is cleared from the QA queue
10.4.4 Customizing QA Thresholds
To Update Thresholds:
- In the QA Review Thresholds section, locate the threshold you want to modify
- Enter the new value (in hours)
- Click Save Changes at the top of the page
Considerations:
- QA Staffing: If you have limited QA staff, you may need longer thresholds to be realistic
- Agency Volume: High-volume agencies may need shorter thresholds to keep up with claim submission deadlines
- Payer Requirements: Some payers require documentation approval within 24-48 hours
- Medicare Compliance: Ensure thresholds allow time for timely OASIS transmission (within 5 days of assessment)
Example Customizations:
- Small Agency (1 QA staff): Increase Normal Visit overdue threshold to 48 hours (more realistic)
- Large Agency (dedicated QA team): Decrease Normal Visit overdue threshold to 24 hours (faster turnaround)
- Strict Compliance Focus: Keep Compliance Visit thresholds at 24/48 hours (no exceptions)
10.4.5 QA Threshold Best Practices
✅ Do This:
-
Monitor Overdue Rates:
- Track what percentage of visits become overdue
- If more than 10-15% are overdue, adjust staffing or thresholds
-
Prioritize Compliance Visits:
- Always review OASIS and recertifications before routine visits
- Use the QA Center's Priority filter to focus on urgent items
-
Notify QA Staff Proactively:
- Set up email or SMS notifications for overdue items
- Send daily digests to QA staff: "You have X visits pending review"
-
Review Threshold Effectiveness:
- Quarterly, review whether thresholds are realistic
- Adjust based on QA staff feedback and performance data
-
Escalate Priority Items:
- When priority threshold is reached, assign a supervisor to review immediately
- Document reasons for delays (e.g., missing physician signature, clinician unavailable for questions)
❌ Avoid This:
-
Don't Set Unrealistic Thresholds:
- Thresholds that are too short create false urgency and stress
- QA staff become desensitized to "overdue" alerts if they're always triggered
-
Don't Ignore Overdue Notifications:
- Overdue items impact billing and compliance
- Address overdue items before starting new reviews
-
Don't Blame QA Staff for Systemic Issues:
- If overdue rates are high, investigate root causes:
- Is documentation quality poor (requiring extensive corrections)?
- Are clinicians submitting notes late?
- Is QA staff understaffed?
- If overdue rates are high, investigate root causes:
10.5 Saving Clinical Settings
10.5.1 How to Save
After making any changes to:
- Documentation Standards
- Vital Sign Thresholds
- QA Review Thresholds
Click the "Save Changes" button in the top-right corner of the page.
What Happens:
- All changes are saved immediately
- A Success toast notification appears: "Clinical settings updated successfully"
- Changes take effect system-wide for all users
10.5.2 Impact of Changes
Documentation Standards:
- New timelines apply to all future visits completed after the change
- Existing visits retain their original timelines (not retroactively changed)
Vital Sign Thresholds:
- New thresholds apply immediately to all future documentation
- Existing vital signs are not re-evaluated (alerts are not retroactively triggered)
QA Review Thresholds:
- New thresholds apply to all future submissions
- Existing items in the QA queue retain their original due dates
10.6 Troubleshooting Common Issues
Issue 1: "Visit Notes Overdue Alert Too Frequent"
Problem: Clinicians are receiving too many "overdue visit note" alerts
Solution:
- Review your Visit notes must be completed within setting
- If set to 24 hours and clinicians work varied schedules, consider extending to 48 hours
- Train clinicians on the importance of timely documentation
- Identify clinicians with frequent overdue notes (may need coaching)
Issue 2: "Vital Sign Alerts Are Too Sensitive"
Problem: Clinicians complain that every vital sign triggers an alert
Solution:
- Review your thresholds in Clinical Alerts & Triggers
- Compare to clinical standards (e.g., American Heart Association guidelines)
- Consider your patient population (elderly patients may have different normal ranges)
- Adjust thresholds to be less sensitive (e.g., increase high BP alert from 140 to 160 mmHg)
- Train clinicians to document accurate vital signs (errors cause false alerts)
Issue 3: "QA Queue Always Overdue"
Problem: Most items in the QA queue are marked as overdue
Solution:
- Check QA Staffing: Do you have enough QA staff for your agency's volume?
- Adjust Thresholds: Increase overdue threshold from 40 to 48 or 72 hours (be realistic)
- Prioritize: Ensure QA staff focus on compliance visits first, then routine visits
- Review Documentation Quality: Are clinicians submitting complete, accurate notes? Poor quality notes take longer to review.
- Automate Where Possible: Use soft alerts and auto-approval for low-risk visits (if your subscription allows)
Issue 4: "Cannot Save Clinical Settings"
Error Message: "Failed to save clinical settings"
Solution:
- Check your internet connection
- Verify you have Agency Administrator role (only admins can change clinical settings)
- Ensure all fields have valid values (numbers only, no text)
- Try refreshing the page and re-entering changes
- Contact Betasky Support if the issue persists
10.7 Best Practices
✅ Do This:
-
Review Settings Quarterly:
- Clinical standards and regulations change
- Review and update thresholds every 3-6 months
-
Align with Agency Policies:
- Ensure settings match your clinical policy manual
- Train staff on the rationale behind each setting
-
Consult Clinical Leadership:
- Involve your Director of Nursing, Medical Director, and QA Manager in setting thresholds
- Get buy-in from clinical staff before implementing changes
-
Monitor Compliance:
- Track how often thresholds are exceeded
- Use data to identify training needs or staffing gaps
-
Document Rationale:
- Keep a record of why you chose specific thresholds
- Useful for state surveys and audits
❌ Avoid This:
-
Don't Set and Forget:
- Settings should be reviewed and adjusted regularly
- Outdated settings can harm compliance and patient safety
-
Don't Ignore Staff Feedback:
- If clinicians or QA staff report issues, investigate and adjust
- Settings should support workflow, not hinder it
-
Don't Copy Another Agency's Settings:
- Each agency has unique patient populations, staffing, and workflows
- What works for another agency may not work for yours
-
Don't Use Extreme Values:
- Setting vital sign thresholds too wide or too narrow defeats their purpose
- Use clinical evidence and guidelines