Chapter 21: QA Center & Review Workflow
Overview
The QA (Quality Assurance) Center is the centralized hub where agency managers and QA reviewers approve, return, or remove clinical documents before they are finalized. Every completed visit form and OASIS assessment must pass through QA review to ensure accuracy, compliance, and quality before being submitted to payers or CMS.
What You'll Learn:
- How documents enter the QA queue and what the dashboard shows
- Understanding the queue table columns (Alerts, Time in Queue, Priority)
- How to run validation checks for OASIS assessments
- Understanding CMS Fatal Errors, Warnings, and Clinical Alerts (Soft Alerts)
- How to approve, return, or remove documents
- Special workflows for documents awaiting physician signature
21.1 Understanding the QA Center Dashboard
When Documents Enter the QA Queue
Documents automatically appear in the QA Center when:
- Visit Forms: A clinician completes a visit note (SN, LPN, HHA, PT, OT, SLP, MSW, Supervisory, Wound Care, etc.)
- OASIS Assessments: A clinician completes an OASIS SOC, Recert, ROC, Transfer, Discharge, Transfer-Discharge, or Death assessment
- Status: The document's status is "Pending Review" or "Pending Physician Signature"
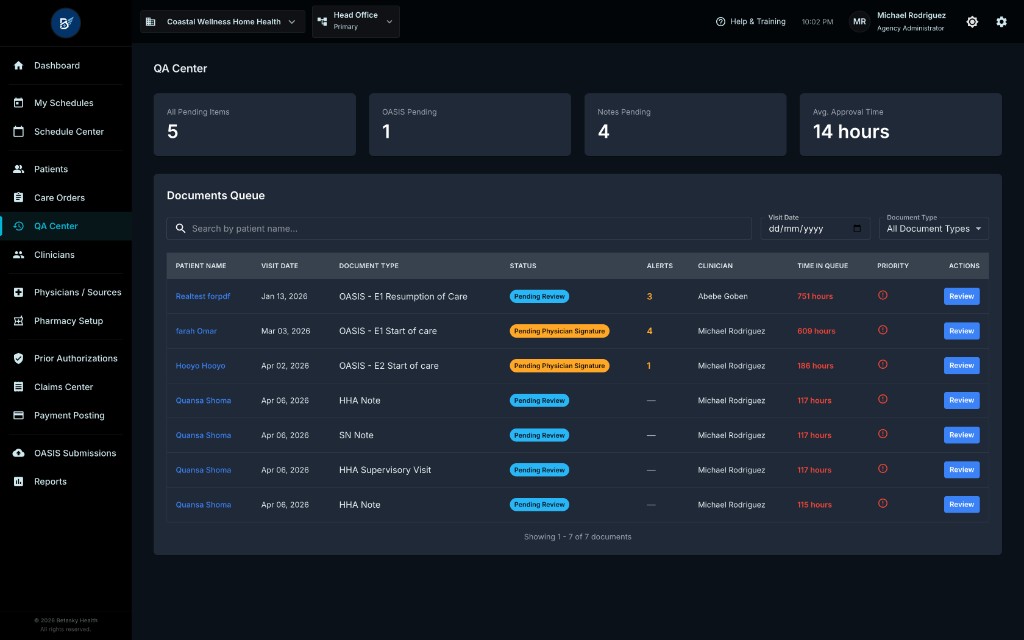
Key Elements on This Screen:
-
Statistics Cards (Top Row):
- All Pending Items: Total number of documents waiting for QA review across all types
- OASIS Pending: Number of OASIS assessments (SOC, Recert, ROC, Transfer, Discharge, etc.) in the queue
- Notes Pending: Number of visit notes (SN, LPN, HHA, PT, OT, SLP, MSW, etc.) in the queue
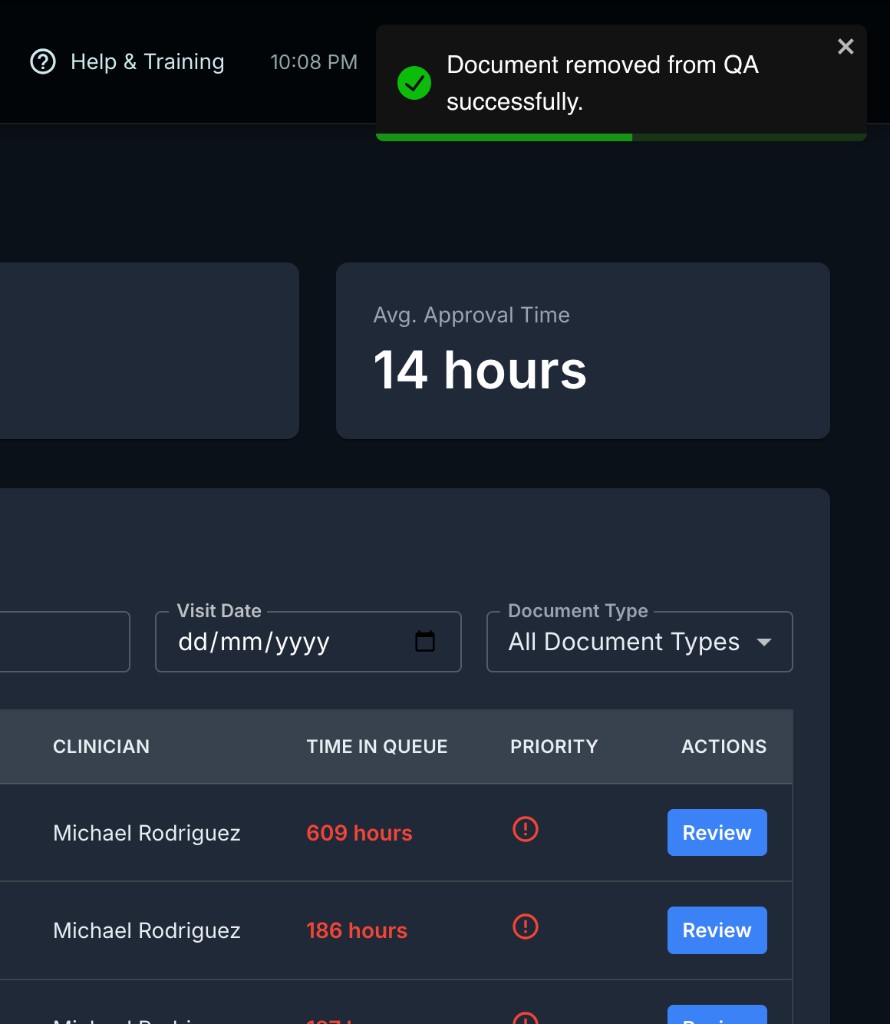
- Avg. Approval Time: Average time it takes for documents to be reviewed and approved (measured in hours). This helps agencies track QA efficiency.
-
Documents Queue Table: A detailed list of all pending documents with powerful filtering and search capabilities
21.2 The Documents Queue Table (Deep Dive)
The queue table is where you manage all pending documents. Each column serves a specific purpose:
Columns Explained in Detail
1. Patient Name
- Displays the patient's first and last name as a clickable link
- Clicking the name takes you directly to the document review page
- Warning Icon: If you see a yellow warning icon next to the name, this is a Missed Visit document. The clinician documented a visit that was marked as "Missed" in the system.
2. Visit Date
- The scheduled date of the visit or assessment (format: MMM dd, yyyy, e.g., "Jan 13, 2026")
- For OASIS assessments, this is the date the assessment was performed
- Use the Visit Date filter above the table to narrow down documents by a specific date
3. Document Type
- Shows the type of clinical document:
- OASIS Forms: "OASIS - E1 Resumption of Care," "OASIS - E2 Start of care," "OASIS - E1 Recertification," etc.
- Visit Notes: "SN Note," "HHA Note," "HHA Supervisory Visit," "PT Visit," "Wound Care Note," etc.
- "Missed" Chip: If a visit was marked as "Missed" by the system, you'll see a yellow "Missed" chip next to the document type
- Use the Document Type dropdown filter to show only specific types (e.g., "All Document Types," "OASIS," "SN," "HHA")
4. Status
- The current review status of the document:
- Pending Review (Blue chip): The document is ready for QA to review and approve or return
- Pending Physician Signature (Orange/Warning chip): The document has been approved by QA but is waiting for the physician to sign it (applies only to OASIS SOC, Recert, and ROC). Once the physician signs, the Care Order becomes "Active."
5. Alerts (Critical Column)
- What This Shows: The total number of validation issues found the last time QA clicked "QA Review" (Check for Errors) on this document
- Alert Count = CMS Fatal Errors + CMS Warnings + Clinical Alerts (Soft Alerts)
- Display:
- Number in Orange: If there are alerts (e.g., "3"), they are shown in bold orange, indicating issues to review
- "—" (Dash): QA has not yet clicked "QA Review" for this document, so no validation has been run
- "0": QA ran validation, and no issues were found
Important: This alert count is cached from the last QA Review scan. If the clinician edits the document after QA initially reviewed it, the alert count won't automatically update. QA must click "QA Review" again to refresh the count.
Why This Matters:
- You can prioritize high-alert documents first
- If a document shows "5" alerts, you know to expect validation issues when you review it
- If alerts are "—", you should run "QA Review" before approving to catch any issues
6. Clinician
- The name of the clinician who completed the document (e.g., "Michael Rodriguez, RN" or "Abebe Geben, PT")
- If the clinician is unassigned or unknown, it shows "Unassigned" or "Unknown"
7. Time in Queue (Critical Column)
- What This Shows: How long the document has been waiting for QA review since it was submitted
- Calculation: Time is measured from the
submittedAttimestamp (when the clinician completed the form) to the current time, displayed in hours (e.g., "751 hours," "800 hours," "117 hours") - Color Indicators:
- Red Text (Bold): The document is Overdue (exceeds the agency's overdue threshold). For most documents, this is after 72 hours (3 days). For compliance documents, it may be 24 hours.
- Black Text (Normal): The document is within the normal timeframe
How Time Thresholds Work (Behind the Scenes):
- Your agency has two types of documents:
- Normal Documents (visit notes, non-compliance OASIS): Overdue threshold is typically 72 hours
- Compliance Documents (OASIS SOC, Discharge, Transfer, Death): Overdue threshold is typically 24 hours (stricter timeline due to regulatory deadlines)
- These thresholds are configurable in Clinical Settings by your administrator
Why This Matters:
- Red, overdue documents should be reviewed immediately to avoid delays in billing or regulatory submissions
- Sorting by "Time in Queue" helps you tackle the oldest documents first
8. Priority (Critical Column)
- What This Shows: A red alert icon appears if the document has been in the queue for a critically long time
- How It Works:
- Normal documents: Priority icon appears after ~48 hours (agency-configurable)
- Compliance documents: Priority icon appears after ~12 hours (stricter)
- Display:
- Red Circle Icon with "!": Document is flagged as Priority and needs immediate attention
- Empty: Document is not yet priority
Why This Matters:
- Priority flags help you identify documents that are at risk of missing deadlines
- You can quickly scan the queue for red icons and tackle those first
- Combined with "Time in Queue," this ensures critical documents don't get lost in the queue
9. Actions
- Review Button (Blue): Clicking this takes you to the detailed document review page where you can:
- View the complete clinical form
- Run validation checks (for OASIS)
- Approve, return, or remove the document
21.3 Filtering and Searching the Queue
The QA Center provides powerful filters to help you manage large volumes of documents:
Search by Patient Name
- Type any part of the patient's first or last name in the "Search by patient name..." box
- The table updates instantly to show only matching patients
- Example: Typing "Real" will show "Realtest Forpdf"
Filter by Visit Date
- Click the Visit Date calendar picker
- Select a specific date to show only documents from that day
- This is useful when reviewing documents from a specific day's schedule
Filter by Document Type
- Click the Document Type dropdown
- Options include:
- All Document Types: Show everything
- OASIS: Show only OASIS assessments (SOC, Recert, ROC, Transfer, Discharge, etc.)
- SN, HHA, PT, OT, SLP, MSW, etc.: Show only specific visit note types
- The system automatically extracts unique document types from your queue
Pro Tip: Use filters together. For example, filter by "OASIS" + a specific date to review all assessments from that day.
21.4 Reviewing a Document
When you click the "Review" button for any document, you're taken to the Document Review Page.
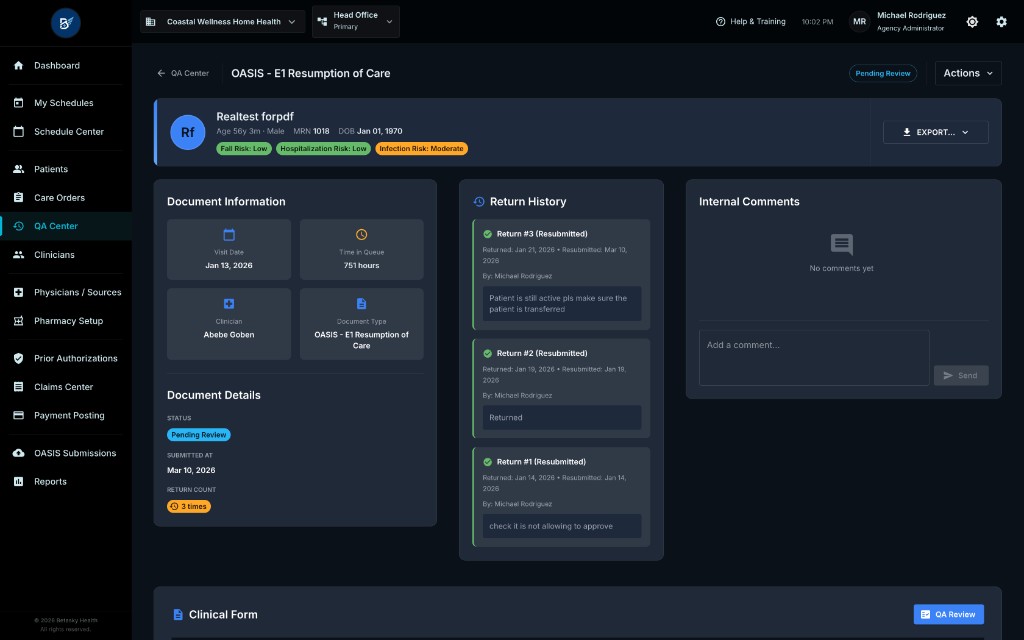
What You See:
-
Top Bar:
- Back Arrow: Returns to the QA Center queue
- Patient Name & Basic Info: Patient's name, age, gender, MRN, DOB, risk indicators (Fall Risk, Hospitalization Risk, etc.)
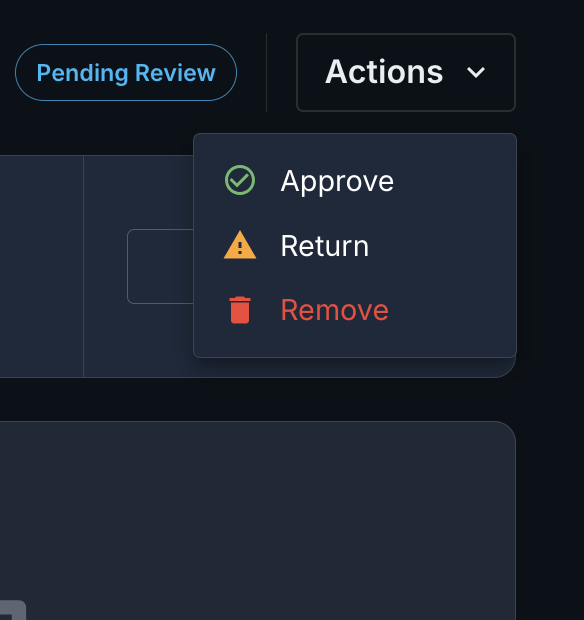
- Status Badge: "Pending Review" or "Pending Physician Signature"
- "Pending Review" Status Indicator (Top Right): Shows the current workflow state
- Actions Dropdown: "Approve," "Return," "Remove" (we'll cover these in detail below)
-
Left Side (Document Information & Return History):
- Visit Date: When the visit or assessment occurred
- Time in Queue: How long it's been since submission
- Clinician: Who completed the document
- Document Type: Full document name (e.g., "OASIS - E1 Resumption of Care")
- Return History (If Applicable): If this document has been returned to the clinician before, you'll see a list of all previous returns with:
- Return date and time
- Reviewer who returned it
- Reason for return (review notes)
-
Right Side (Internal Comments):
- Comments Area: QA team members can leave internal notes for each other about this document
- Add a Comment: Type a note and click "Send" to add it
- Delete Comment: If you authored a comment, you can delete it
- Use Cases:
- "Spoke with clinician about missing medication review - will update by EOD"
- "Flagged for follow-up on wound measurement discrepancy"
- "Waiting for physician callback to verify diagnosis code"
-
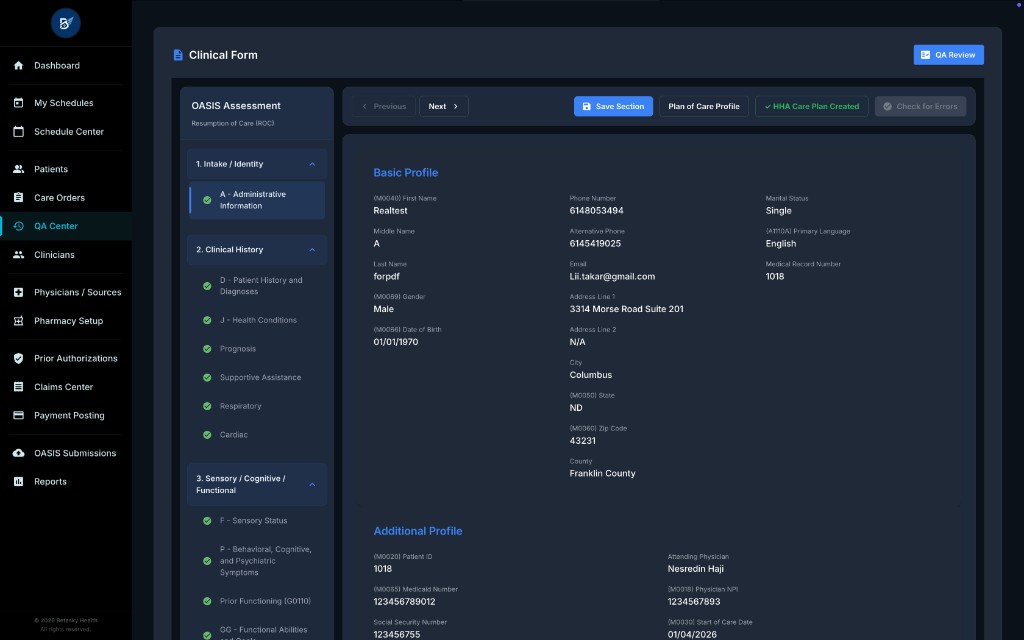
Clinical Form Section (Bottom):
- "QA Review" Button (Blue, For OASIS Only): Clicking this runs a comprehensive validation check on the OASIS assessment. We'll cover this in the next section.
- Form Content: The actual clinical document is displayed in read-only mode. You can scroll through all sections to review the clinician's documentation.
21.5 Running "QA Review" (Validation Check for OASIS)
For OASIS assessments only, the system provides a powerful "QA Review" button that scans the entire form for errors and clinical inconsistencies.
What Happens When You Click "QA Review":
-
The Button Changes:
- Button text changes to "Scanning…" with a spinning loader
- The system is now checking the OASIS assessment against three types of validation:
-
Three Validation Checks Run Simultaneously:
a. Agency Required Fields Check:
- The system checks if all fields marked as "required" by your agency's internal policy are filled in
- These are fields your agency has designated as mandatory beyond what CMS requires
- Example: Your agency may require a detailed social history note for all SOC assessments
b. CMS Validation Check (Fatal & Warnings):
- Fatal Errors: CMS edit rules that MUST be fixed before the assessment can be submitted to CMS. If any fatal errors exist, the document cannot be finalized.
- Warnings: CMS edit rules that flag potential issues but do not block submission. These are advisory and should be reviewed, but you can proceed if the clinician has a valid reason.
- Examples of CMS errors:
- "Use sequence error: Info Completed Date (M0090/M0100) cannot be before Start of Care Date (M0030/M0032)"
- "Date of Birth (M0066) – Year of Birth must be within 5 days of Start of Care Date (M0030)"
- "Height Out of Expected Range (SA.SOC.NUTR.048): Patient height (Weight: 8lbs) is outside expected range (80-64 inches). Verify measurement."
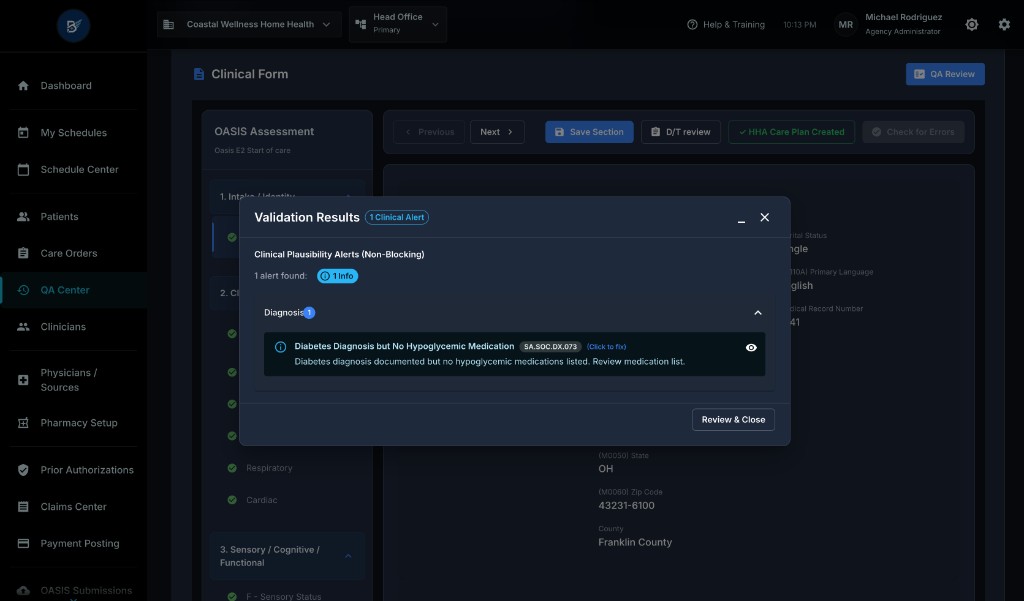
c. Clinical Plausibility Alerts (Soft Alerts):
- The system runs soft alerts, which are non-CMS, clinical plausibility checks to flag unusual or inconsistent documentation
- These are INFO or WARN level alerts, not errors. They are advisory and meant to help QA catch potential mistakes or prompt clinician clarification.
- Examples:
- Grooming vs Dressing Inconsistency (SA.SOC.FUNC.001): "Patient needs assistance with grooming (M1810=1) but is independent with dressing (M1830=0, M1840=0). This is clinically unusual."
- Bowel Incontinence Toileting Independence (SA.SOC.ELIM.038): "Patient has severe transfer limitations (M1850=3) but no pressure ulcer documented. High-risk population."
- No Signed Medication Review (SA.SOC.MEDS.074B): "Patient is on hypoglycemic medications but no signed medication review is documented. Review medication profile for drug interaction check."
-
Validation Results Modal Opens:
What You See in This Modal:
-
Modal Title: "Validation Results"
-
Chips at the Top (Summary):
- "1 Clinical Alert" (Blue Chip): Shows the count of soft alerts
- If there were fatal errors: "X CMS Fatal" (Red Chip)
- If there were warnings: "X Warnings" (Orange Chip)
- If there were agency required field issues: "X Required Fields" (Red Chip)
-
Minimize Button (Top Right, "—" icon): Clicking this minimizes the modal to a small draggable box in the corner. This allows you to review the form and navigate to specific fields while keeping the validation results visible. Click the minimized box to expand it again.
-
Close Button (Top Right, "X" icon): Closes the modal entirely
21.6 Understanding Validation Error Types (In-Depth)
When you run "QA Review," the modal displays errors in sections by severity. Let's break down each type:
Section 1: Agency Required Fields (Red Alert Box)
What This Means:
- These fields are mandatory by your agency's policy, even if CMS doesn't require them
- Must be completed before you can approve the document
- Example message: "Agency Required: Social History narrative is missing (Intake > Demographics). Complete this section before approval."
What You Do:
- Click "Close & Fix Errors"
- The modal closes, and you can see the form below
- Scroll to the section mentioned (or use the navigation if provided)
- Return the document to the clinician with a clear note explaining what's missing
Section 2: HHA Care Plan Required (Red Alert Box)
What This Means:
- For OASIS SOC and ROC assessments, if the Plan of Care includes HHA (Home Health Aide) orders with frequency > 0, the clinician MUST create an active HHA Care Plan before completing the assessment
- This is a system-enforced rule to ensure HHAs have documented instructions
Example Message:
- "HHA services are ordered. You must create the HHA Care Plan before finalizing this assessment."
What You Do:
- Return the document to the clinician with a note: "HHA Care Plan is missing. Please create the HHA Care Plan from the 'HHA Care Plan' button on the OASIS form before resubmitting."
Section 3: CMS Fatal Errors (Red Alert Box)
What This Means:
- These are CMS edit rule violations that will cause the OASIS assessment to be rejected by CMS if submitted
- Must be fixed before finalizing the document
- Each error shows:
- Error Message: Human-readable description of the issue
- CMS Edit ID: The official CMS edit code (e.g., "CMS Edit -3060," "SA.SOC.FUNC.001")
- Item Code: The OASIS item that failed (e.g., "M0100," "M1810," "GG0130A")
- "(Click to fix)" Link: If available, clicking this link navigates directly to the problematic field in the form (only works when the modal is minimized or closed)
Examples of CMS Fatal Errors:
-
Date Sequence Error:
- Message: "Use sequence error: Info Completed Date (M0090/M0100) cannot be before Start of Care Date (M0030/M0032)."
- Meaning: The clinician entered an assessment completion date that is earlier than the start of care date. This is logically impossible.
- What to do: Return the document with a note: "Please correct the dates. The assessment completion date (M0100) must be on or after the Start of Care date (M0030)."
-
Grooming vs Dressing Inconsistency:
- Message: "Grooming vs Dressing Inconsistency (SA.SOC.FUNC.001): Patient needs assistance with grooming (M1810=1) but is independent with dressing (M1830=0, M1840=0). This is clinically unusual."
- Meaning: It's rare for a patient to need help with grooming but be fully independent with dressing. This may indicate a documentation error.
- What to do: Return with a note: "Please review functional status documentation. It's unusual for a patient to need grooming assistance but be independent with dressing. Verify these values."
-
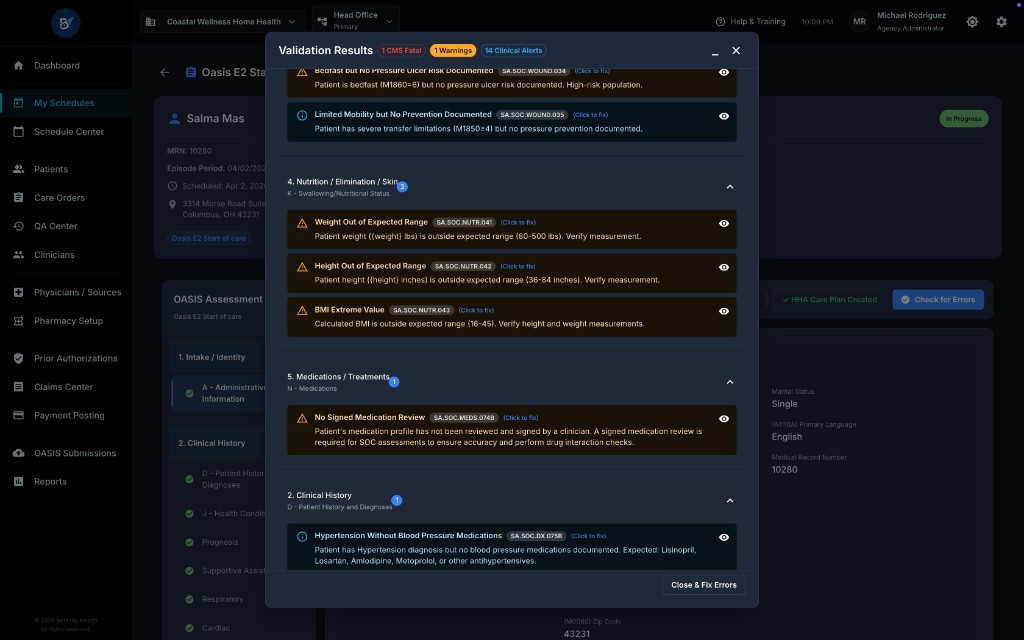
Weight Out of Expected Range:
- Message: "Weight Out of Expected Range (SA.SOC.NUTR.048): Patient weight (Weight: 8lbs) is outside expected range (80-200 lbs). Verify measurement."
- Meaning: The entered weight is implausibly low (8 lbs for an adult is clearly a typo).
- What to do: Return with a note: "Patient weight is entered as 8 lbs, which is incorrect. Please verify and update the weight measurement."
What You Do:
- Read each fatal error carefully
- If you can see the form below (or minimize the modal), navigate to the problematic field to understand the issue
- Return the document to the clinician with a clear, specific note for each error
Section 4: Warnings (Orange Alert Box)
What This Means:
- These are CMS warnings, not fatal errors
- They do not block submission to CMS, but they flag potential issues
- You can approve the document even if warnings exist, but you should review them
Example Warning:
- Message: "For SOC, Date Assessment Completed should be within 5 days of Start of Care Date (M0030). Current gap: 14 days."
- Meaning: CMS recommends completing the SOC assessment within 5 days of the start of care date. This assessment was completed 14 days later. CMS will accept it, but it's outside the recommended timeframe.
What You Do:
- Review the warning and decide:
- If it's explainable: (e.g., the patient was hospitalized during that window, delaying the assessment), you can approve with an internal comment noting the reason
- If it seems wrong: Return to the clinician with a note: "Assessment was completed 14 days after SOC. Please verify the completion date or provide a note explaining the delay."
Section 5: Clinical Plausibility Alerts (Soft Alerts) (Blue Info Box)
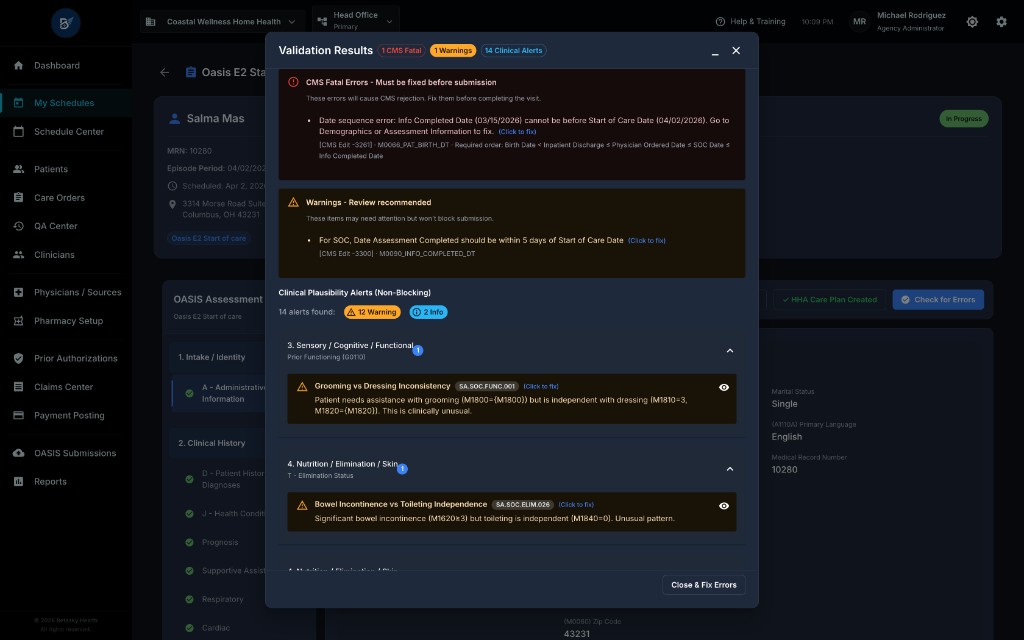
What This Means:
- These are non-CMS, clinical plausibility checks designed to catch unusual or inconsistent documentation
- They are informational or warning level and do not block approval
- Soft alerts are grouped into packs (categories) like:
- FUNC (Functional Status)
- NEURO (Neuro/Cognition)
- GG (GG Functional Abilities)
- ELIM (Elimination Status)
- WOUND (Wound/Integumentary)
- NUTR (Nutrition)
- MEDS (Medications)
- SUPP (Supportive Assistance)
- DX (Diagnosis)
- CROSS (Cross-Module Checks)
How Soft Alerts Are Displayed:
- The modal shows a collapsible section titled "Clinical Plausibility Alerts (Non-Blocking)"
- Each pack (e.g., "FUNC," "MEDS") has a header showing the number of alerts in that category
- Click the header to expand and see individual alerts
Example Soft Alerts:
-
Grooming vs Dressing Inconsistency (FUNC Pack, SA.SOC.FUNC.001):
- Severity: INFO
- Message: "Patient needs assistance with grooming (M1810=1) but is independent with dressing (M1830=0, M1840=0). This is clinically unusual."
- Evidence: Shows the exact OASIS items and their values (e.g., "M1810: Current Ability to Dress Upper Body Safely = 1 - Requires minimal assistance")
- Recommended Actions:
- "Review functional status assessment with clinician"
- "Verify patient is truly independent with dressing if grooming requires assistance"
- "Consider if grooming includes specialized tasks (e.g., oral care) that may explain the discrepancy"
-
Diabetes Diagnosis but No Hypoglycemic Medication (MEDS Pack, SA.SOC.MEDS.075A):
- Severity: WARN
- Message: "Patient has Diabetes diagnosis (ICD-10: E11.9) but no hypoglycemic medications documented. Review medication list."
- Evidence: Shows the diagnosis code and the absence of hypoglycemic medication classes in the patient's medication profile
- Recommended Actions:
- "Verify patient is not on insulin or oral hypoglycemic agents"
- "If patient is diet-controlled, document this in the clinical notes"
- "Review with clinician if medication list is incomplete"
-
No Signed Medication Review (MEDS Pack, SA.SOC.MEDS.074B):
- Severity: WARN
- Message: "Patient is on hypoglycemic medications but no signed medication review is documented. Review medication profile for drug interaction check."
- Evidence: Shows that the patient is on medications requiring interaction checks, but no signed medication review exists in the system
- Recommended Actions:
- "Complete a signed medication review in the Medication Profile"
- "Perform drug interaction check (required for SOC per CMS guidance)"
- "Document any identified interactions or contraindications"
What You Do with Soft Alerts:
- Review them carefully to understand if they flag real issues or are explainable
- INFO Alerts: These are minor inconsistencies. If they seem reasonable, you can approve without action. If they seem wrong, return to the clinician with a note.
- WARN Alerts: These are more significant clinical concerns. You should either:
- Verify the clinician's documentation is correct (e.g., call the clinician to discuss)
- Return the document with a note asking for clarification or correction
- Add an internal comment documenting why you're approving despite the alert
Pro Tip: Soft alerts are learning tools. Over time, they help clinicians improve documentation quality and catch mistakes before they become billing or compliance issues.
21.7 Approving, Returning, or Removing Documents
After reviewing the document and (for OASIS) running validation checks, you have three actions:
Action 1: Approve
When to Use:
- The document is complete, accurate, and meets all requirements
- For OASIS: No fatal errors exist (warnings and soft alerts are acceptable if explainable)
- The clinician's documentation is clear and clinically sound
How to Do It:
- Click the "Actions" dropdown (top right of the review page)
-
Select "Approve"
-
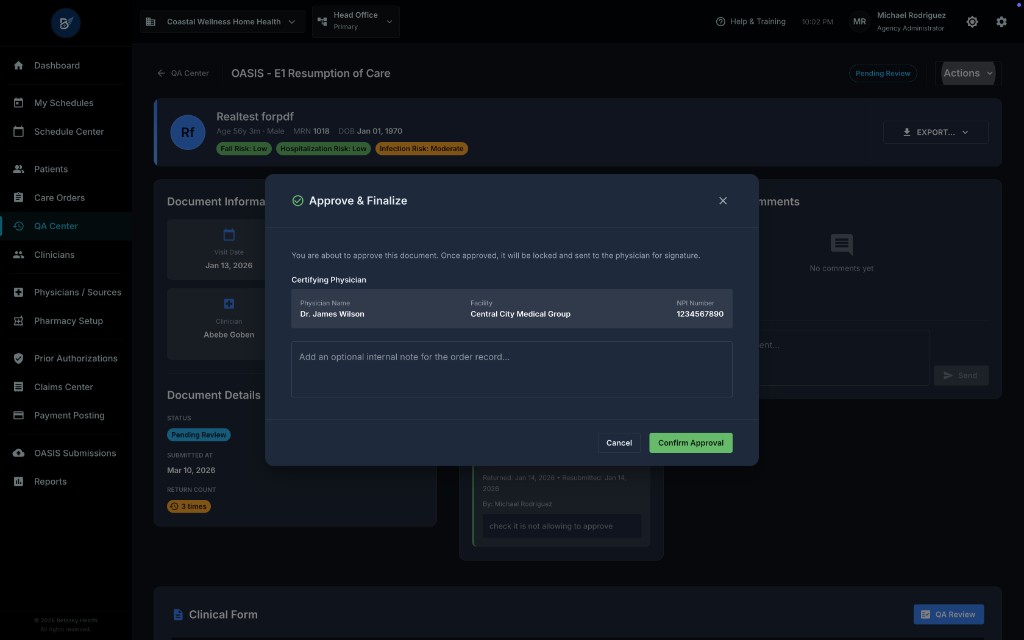
The "Approve & Finalize" modal appears:
What You See:
- Modal Title: "Approve & Finalize"
- Message: "You are about to approve this document. Once approved, it will be locked and sent to the physician for signature." (This message varies depending on the document type. For non-OASIS documents, it may say "locked and finalized.")
- Certifying Physician Info (For OASIS SOC/Recert/ROC): Shows the physician name, facility, and NPI number who will need to sign the document
- Optional Internal Note Field: You can add a note for the care order record (e.g., "Approved after clinician corrected medication list")
- Cancel Button: Returns to the review page without approving
- "Confirm Approval" Button (Green): Completes the approval
- Click "Confirm Approval"
What Happens After Approval:
-
For OASIS SOC, Recert, ROC:
- Status changes to "Pending Physician Signature"
- The document is locked (clinician and QA cannot edit it)
- A notification is sent to the certifying physician to sign the document electronically
- Once the physician signs, the Care Order status changes to "Active" (for SOC) or a new 60-day episode begins (for Recert)
- The document moves out of the QA queue
-
For OASIS Transfer, Discharge, Transfer-Discharge, Death:
- Status changes to "Approved" (final status, no physician signature required)
- The document is locked
- "Safety Sweep" Actions Occur Automatically:
- Transfer: Care Order status changes to "ON_HOLD", all scheduled visits are canceled, prior authorizations are paused
- Discharge: Care Order status changes to "CLOSED", all scheduled visits are canceled, prior authorizations are closed
- Death: Patient status changes to "DECEASED", Care Order closes, all visits/PAs canceled
- The document moves out of the QA queue
-
For Visit Notes (SN, LPN, HHA, PT, OT, SLP, MSW, etc.):
- Status changes to "Approved"
- The document is locked (no further edits)
- A medication snapshot is taken (a frozen copy of the patient's medication list at the time of approval, for billing and compliance)
- The visit is marked as "Completed" in the schedule
- The document moves out of the QA queue
Action 2: Return for Correction
When to Use:
- The document has errors that the clinician needs to fix
- Documentation is incomplete or unclear
- You have questions that require clinician clarification
How to Do It:
-
Click the "Actions" dropdown
-
Select "Return"
-
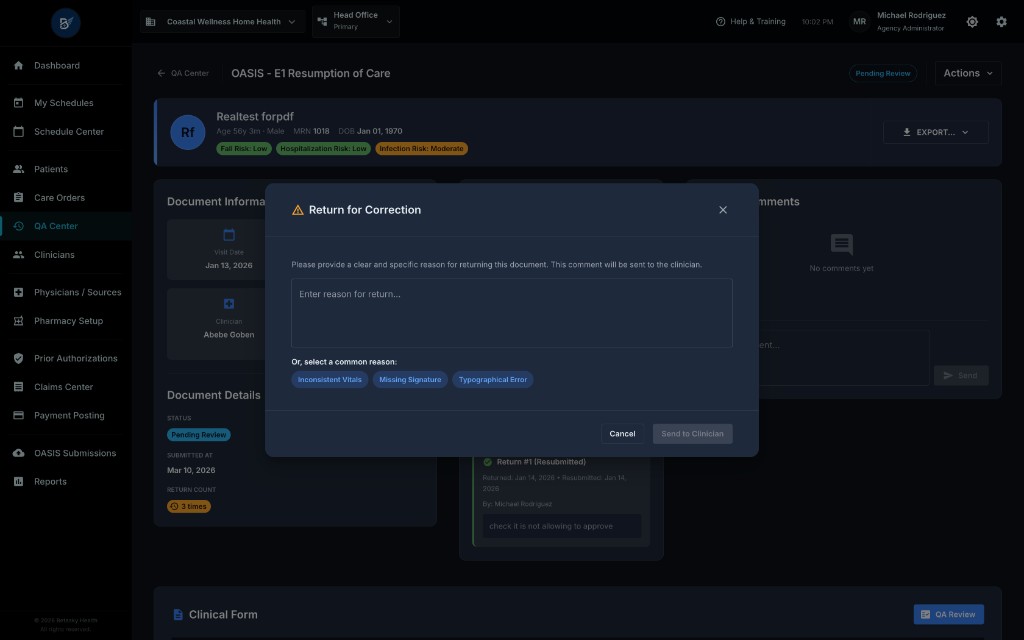
The "Return for Correction" modal appears:
What You See:
- Modal Title: "Return for Correction"
- Message: "Please provide a clear and specific reason for returning this document. This comment will be sent to the clinician."
- Reason Text Area: A large text box where you type your feedback
- Common Reason Chips (Shortcuts): Pre-written reasons you can click to auto-fill:
- "Inconsistent Vitals"
- "Missing Signature"
- "Typographical Error"
- "Or, select a common reason:" Section: Quick-select buttons for common issues
- Cancel Button: Returns to the review page without returning the document
- "Send to Clinician" Button (Orange): Completes the return
-
Type a Clear, Specific Reason:
- Bad Example: "Fix errors"
- Good Example: "Please correct the following errors:
- Patient weight is entered as 8 lbs (M1060) – verify and update.
- Assessment completion date (M0100) is before the Start of Care date (M0030) – adjust dates.
- HHA Care Plan is missing – create the care plan from the OASIS form before resubmitting."
-
Click "Send to Clinician"
What Happens After Returning:
- Status changes to "Returned for Correction"
- The clinician receives a notification (email and/or in-app alert) that the document was returned
- The document leaves the QA queue temporarily
- The clinician can edit the document to fix the issues
- Return count increments: The system tracks how many times a document has been returned (shown in the "Return History" section on the review page)
- When the clinician resubmits, the document re-enters the QA queue with status "Pending Review"
Pro Tip: Be specific and kind in your return notes. Clear feedback helps clinicians learn and reduces the number of re-returns.
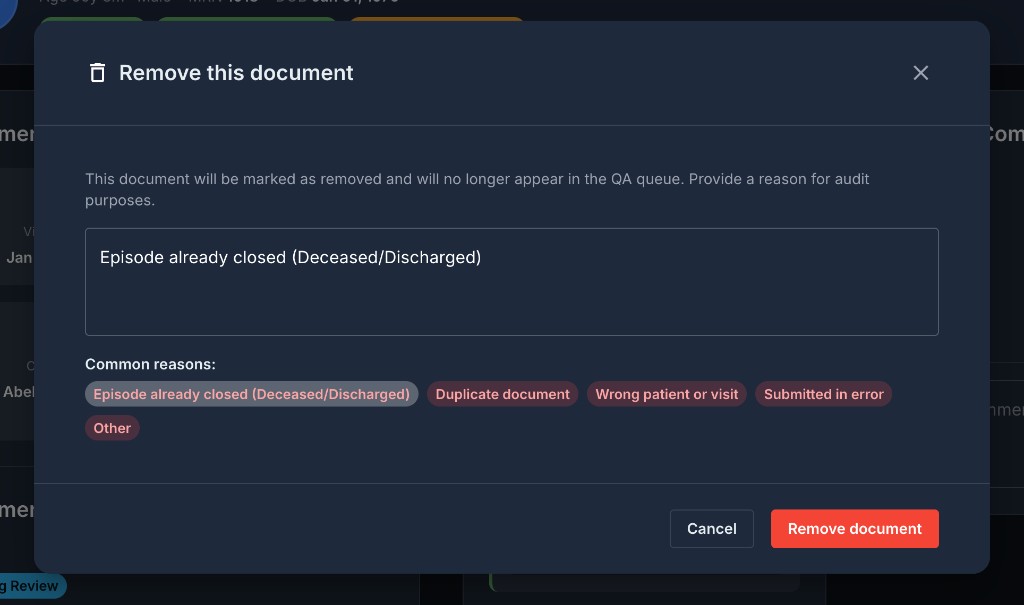
Action 3: Remove from QA
When to Use (Rare):
- The document should not have been submitted to QA in the first place
- The episode or care order has been closed, discharged, or deceased, making the document obsolete
- The document is a duplicate
- The visit was entered in error and should be deleted
How to Do It:
-
Click the "Actions" dropdown
-
Select "Remove"
-
The "Remove this document" modal appears:
What You See:
- Modal Title: "Remove this document"
- Warning Message: "This document will be marked as removed and will no longer appear in the QA queue. Provide a reason for audit purposes."
- Reason Text Area: Type the reason for removal
- Common Reasons (Chips):
- "Episode already closed (Deceased/Discharged)"
- "Duplicate document"
- "Wrong patient or visit"
- "Submitted in error"
- "Other"
- Cancel Button: Returns to the review page without removing
- "Remove document" Button (Red): Completes the removal
- Type a Clear Reason for Audit Purposes
- Click "Remove document"
What Happens After Removal:
- Status changes to "Removed"
- The document is marked as removed (not deleted, for audit trail)
- The document leaves the QA queue permanently
- The clinician is NOT notified (unlike a return, removal is a QA-only action)
- The removal reason is logged for compliance and audit purposes
Important: Removing a document does not delete the visit or reverse any clinical data. It only removes the document from the QA workflow. If the visit should not exist, coordinate with the clinician or administrator to delete or reschedule it.
21.8 Special Case: Pending Physician Signature
For OASIS SOC, Recertification, and ROC assessments, after QA approval, the document enters a "Pending Physician Signature" state.
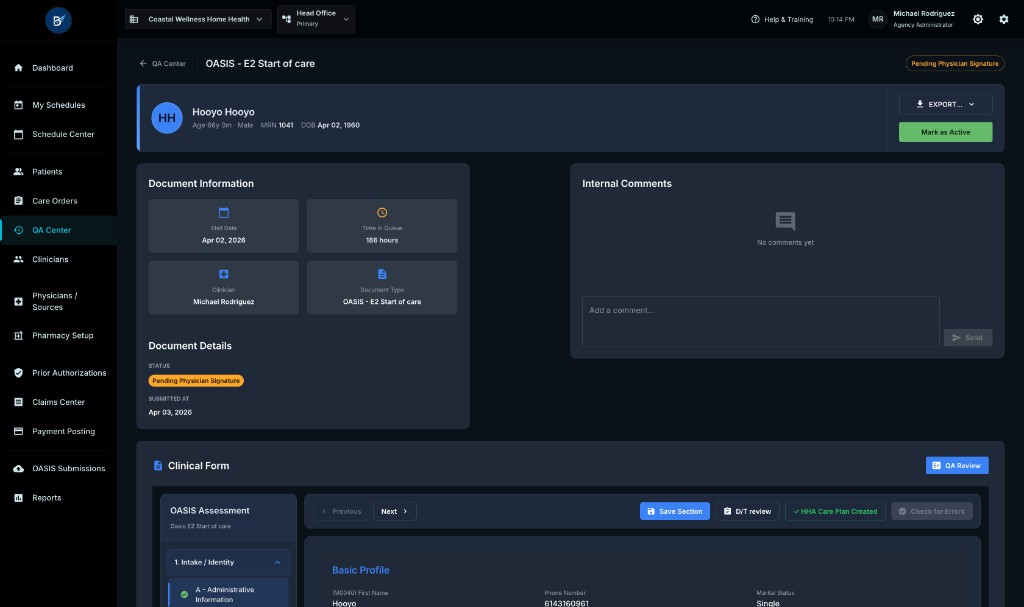
What This Means:
- The document has been approved by QA
- The certifying physician must sign the Plan of Care electronically to activate the care order
- The document remains in this state until the physician signs
Who Can See These Documents:
- These documents stay in the QA queue with status "Pending Physician Signature" (orange/warning chip) so QA can track them
- You can also view them in the Care Order Details > Documents tab
How the Physician Signs:
- The physician logs into the system (or uses a physician portal)
- They navigate to "Documents Awaiting Signature" or receive a notification
- They review the Plan of Care (CMS-485) and OASIS assessment
- They click "Sign" and enter their electronic signature
What Happens After Physician Signs:
- For SOC: The Care Order status changes from "PENDING_POC_SIGNATURE" to "ACTIVE". Home health services can now begin.
- For Recertification: A new 60-day episode is created, and the Care Order remains "ACTIVE" for the new period.
- For ROC: The Care Order returns to "ACTIVE" status after a hospitalization or interruption.
- The document status changes to "Approved" (final status)
- The document leaves the QA queue
QA Role in This Phase:
- You can monitor these documents to ensure physicians sign them promptly
- If a physician is delayed, you can follow up directly or use the system's notification features
- Some agencies have a "Mark as Active" button (visible to administrators) that allows manually activating a care order without physician signature in emergency situations (e.g., physician is unavailable, but services must start). This should be used sparingly and only with proper authorization.
21.9 Export Options (For OASIS Assessments)
For OASIS assessments, you have the option to export the assessment as a PDF for printing, emailing, or archiving.
How to Do It:
- On the document review page, click the "EXPORT…" dropdown (top right, next to the Actions dropdown)
- Select from the available options:
- "OASIS Assessment": Exports the full OASIS assessment as a PDF with all sections, questions, and answers
- "Plan of Care (CMS-485)": Exports the Plan of Care (CMS-485 form) as a PDF, which includes the physician orders, disciplines, frequencies, and goals
What Happens:
- The system generates a PDF document
- Your browser downloads the file automatically
- You can now print it, email it to the physician, or save it to the patient's chart
Use Cases:
- Sending a copy to the physician for review before they sign electronically
- Printing for a paper chart (if your agency maintains both digital and paper records)
- Providing a copy to the patient or family (with appropriate redactions if needed)
- Archiving for compliance or audit purposes
21.10 Best Practices for QA Reviewers
1. Prioritize by Time in Queue and Priority Icon
- Review overdue documents (red text) first
- Tackle priority-flagged documents (red icon) before others
- Use the "Time in Queue" column to sort the queue and work oldest-first
2. Always Run "QA Review" for OASIS Before Approving
- Never approve an OASIS assessment without clicking "QA Review" and reviewing the validation results
- Even if the alert count shows "0," run it yourself to ensure nothing changed since the last scan
3. Be Specific in Return Notes
- Don't just say "fix errors." List each error with its location and what needs to be corrected.
- Example: "1. Correct weight (8 lbs is incorrect - verify). 2. Adjust M0100 date to be after M0030. 3. Create HHA Care Plan."
4. Use Internal Comments for Team Collaboration
- If you're unsure about a document, leave a comment for another QA reviewer: "Can someone else review the wound measurements on this? They seem inconsistent."
- Document decisions: "Approved with soft alert for diabetes medication because patient is diet-controlled (verified with clinician)."
5. Educate Clinicians on Common Errors
- If you see the same errors repeatedly from a clinician (e.g., date sequence errors, missing HHA care plans), schedule a brief training session
- Share examples of good vs. poor documentation
6. Track Your Approval Time
- Use the statistics card ("Avg. Approval Time") to monitor how long documents stay in the queue
- Set agency goals (e.g., "All documents reviewed within 24 hours") and work toward them
7. Don't Rush Soft Alerts
- Soft alerts are non-blocking, but they often flag real clinical issues
- Take a moment to review them and decide if they warrant clinician follow-up
- If you approve with a soft alert, document why in an internal comment
8. Coordinate with Physicians for Pending Signature Documents
- If documents are stuck in "Pending Physician Signature" for more than 48 hours, follow up with the physician's office
- Ensure physicians have access to the system and understand how to sign electronically
21.11 Common Scenarios & How to Handle Them
Scenario 1: Document Shows "5 Alerts" But Clinician Says They Fixed Everything
- What's Happening: The alert count is cached from the last "QA Review" scan. If the clinician edited the document after you initially reviewed it, the alert count won't auto-update.
- What to Do:
- Open the document review page
- Click "QA Review" again to refresh the validation
- If alerts are now "0," proceed with approval
- If alerts still exist, return the document with specific notes
Scenario 2: OASIS SOC Has a Soft Alert for "No Signed Medication Review"
- What's Happening: The system detected that the patient is on medications requiring interaction checks (e.g., hypoglycemic drugs, anticoagulants), but no signed medication review exists in the Medication Profile.
- What to Do:
- Check if the medication review is truly missing (navigate to the patient's Medication Profile)
- If missing: Return the document with a note: "Please complete a signed medication review in the Medication Profile. CMS requires drug interaction checks for SOC assessments."
- If the review exists but wasn't detected: This is a timing issue (review was signed after the OASIS was completed). You can approve with an internal comment: "Medication review completed 1/15/26 - approved."
Scenario 3: Clinician Asks Why Their Document Was Returned When It "Looks Fine"
- What's Happening: The clinician may not understand CMS validation rules or soft alert logic.
- What to Do:
- Schedule a brief call or send a detailed email explaining each error
- Use the exact error messages from the validation modal (including CMS Edit IDs)
- Provide examples of correct documentation
- Offer to review a test document with them to prevent future returns
Scenario 4: Document Has Only Soft Alerts (No Fatal Errors), But Something Feels "Off"
- What's Happening: Soft alerts are designed to catch unusual patterns. Trust your clinical judgment.
- What to Do:
- Review the specific alerts carefully
- If they raise legitimate concerns, call the clinician to discuss
- If the clinician can explain the documentation (e.g., "Patient has upper extremity amputations, so grooming is harder than dressing"), approve with an internal comment documenting the explanation
- If the clinician agrees it's an error, return the document
Scenario 5: Transfer OASIS Is Approved, But Visits Were NOT Canceled
- What's Happening: The "Safety Sweep" (automatic visit/PA cancellation) should happen immediately upon Transfer approval. If it didn't, there's a system issue.
- What to Do:
- Check the Care Order status - it should be "ON_HOLD"
- If visits are still showing as "Scheduled" after approval, contact your system administrator or IT support
- Manually cancel visits if necessary to prevent clinicians from attempting to complete them
21.12 Troubleshooting
Issue: "QA Review" Button Is Not Showing
- Cause: The "QA Review" button only appears for OASIS assessments (SOC, Recert, ROC, Transfer, Discharge, Transfer-Discharge, Death). It does not appear for visit notes (SN, HHA, PT, etc.).
- Solution: For visit notes, you review the form manually without validation checks. No action needed.
Issue: Document Shows "—" in the Alerts Column
- Cause: QA has not yet clicked "QA Review" for this document, so no validation has been run.
- Solution: This is normal for new documents. Click "Review" and then "QA Review" to run validation.
Issue: "Approve" Button Is Grayed Out
- Cause: You may not have permission to approve this document type (some agencies restrict approvals to specific roles), or the document is already approved.
- Solution: Check your user role and permissions with your administrator. If the document status is already "Approved," no action is needed.
Issue: Clinician Says They Never Received the Return Notification
- Cause: The clinician's email address may be incorrect, or email notifications are not configured in the system.
- Solution:
- Verify the clinician's email in their user profile
- Check the system's notification settings with your administrator
- As a workaround, call or text the clinician directly to notify them of the return
Issue: Physician Signature Is Delayed for 48+ Hours
- Cause: The physician may not have received the notification, or they don't have access to the system.
- Solution:
- Check the physician's contact info in the Physicians/Sources module
- Call or email the physician's office to follow up
- Provide the physician with a PDF export (see Section 21.9) if they prefer to review it before signing electronically
- If the physician is unavailable and services must start, consult with your agency administrator about the "Mark as Active" emergency procedure
Issue: Document Is Returned, But It's Not Showing in the Clinician's Queue
- Cause: The clinician may be filtering their visit list and not seeing "Returned for Correction" status.
- Solution: Have the clinician check their My Schedules or My Day page and look for documents with status "Returned for Correction" (usually shown with a yellow/orange chip).